Index
This topic area covers statistics and information relating to young people smoking tobacco and using e-cigarettes in Hull including local strategic need and service provision. Further information relating to Smoking in Pregnancy is given under Maternal Health and Infants within Children and Young People, and Smoking and Vaping Among Adults is given under Lifestyle Factors within Adults. Smoking information has been collected within Hull’s Health and Wellbeing Surveys (both young people and adults) and more recent information on the use of e-cigarettes. The full reports are available under Surveys within Tools and Resources.
Headlines
- Tobacco is a unique product. It is the only consumable that, when used in the intended way, kills half of its users.
- As smoking and deprivation is associated this acerbates the inequalities associated with poverty and deprivation. Smoking is the main contributor to health inequalities. It is estimated that 1.5 million children in the UK are living in circumstances of severe financial deprivation whose plight is exacerbated by parental smoking. It also accounts for approximately half of the difference in life expectancy between the lowest and highest deprivation groups.
- Among secondary school pupils in Hull in 2024, 4.7% of males and 3.1% of females smoked (overall 3.9%). Prevalence increased with age so the highest percentage who smoked was among those aged 15-16 years in school year 11 (15.6% of males and 7.2% of females).
- In 2024, it was estimated that there were 17,376 young people aged 11-16 years living in Hull, and that 673 of them smoked.
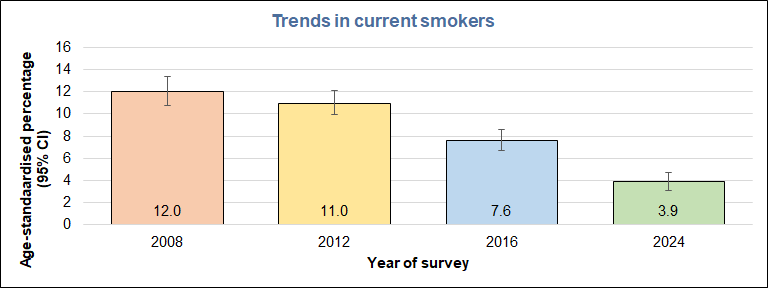
- The smoking prevalence among young people in Hull has decreased dramatically between 2008 and 2024. In 2008, 12% of young people smoked, falling 3.9% in 2024. Despite this large decrease the smoking prevalence is slightly higher in Hull than England, and smoking prevalence is strongly associated with deprivation being around twice as high among young people living in the most deprived fifth of areas of Hull compared to those living in the least deprived fifth of areas of Hull.
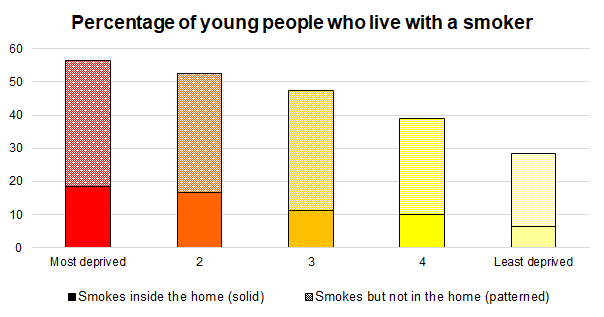
- From the 2016 Health and Wellbeing Survey, just under half of young people in Hull lived with a smoker (57% of young people who lived in the most deprived fifth of areas of Hull compared to 29% of children living in least deprived fifth of areas of Hull). Most smokers start young (two-thirds before the age of 18). Children growing up among smokers are three times more likely to become smokers themselves, and in the local survey, young people living with household members who smoked were much more likely to be occasional or regular smokers (2.1% where no-one smoked in the home, 8.0% where someone smoked but not inside the home, and 14.8% where someone smoked and they smoked inside the home).
- Action on Smoking and Health (ASH) estimate that smoking costs Hull’s society a total of £120 million each and every year. This does not include the cost of Hull smokers purchasing tobacco products which is an estimated £88 million per year.
- In Hull’s Health and Wellbeing Survey conducted during 2016, 7.5% of boys and 9.0% of girls currently vaped, and prevalence increased with age, and was very strongly associated with tobacco smoking. Among those who had never smoked tobacco, 2.2% currently vape, 15.0% had previously vaped and 82.9% had never vaped. However, among regular tobacco smokers, 92.3% currently vape, 3.8% had previously vaped and only 3.9% had never vaped.
- In Hull’s Vaping Survey conducted during 2022, around 14% of boys and girls aged 11-13 years had tried vaping, as had 21.9% of males aged 14-15 years, 27.4% of females aged 14-15 years, 39.4% of males aged 16-17 years and 48.6% of females aged 16-17 years. Whilst the percentage who vaped occasionally or regularly was small among those aged 11-13 years (2.6% for males and 3.3% for females), the percentages were higher among older age groups particularly among females with 5.7% of males aged 14-15 years, 10.1% of females aged 14-15 years, 17.3% of males aged 16-17 years and 28.3% of females aged 16-17 years vaping occasionally or regularly.
- Whilst there was a very strong association between smoking tobacco / cigarettes and vaping, 71% of those who had tried vaping (and who could remember the order) had vaped first or had never smoked tobacco / cigarettes.
- Overall, 37% of young people lived with someone who vaped, including 23% of young people where the person or persons vaped inside the home. There was a strong association between household exposure to vaping and the young person’s experience of vaping.
- The majority used disposable vapes, and most young people who had tried vaping had been using them for a short period of time. Sizable percentages found vapes easy to buy despite it being illegal to sell vapes to under 18s. The majority of young people who vaped regularly or occasionally agreed with ‘I am addicted to vapes’ and often or sometimes craved a vape or felt irritable if they hadn’t vaped for a while.
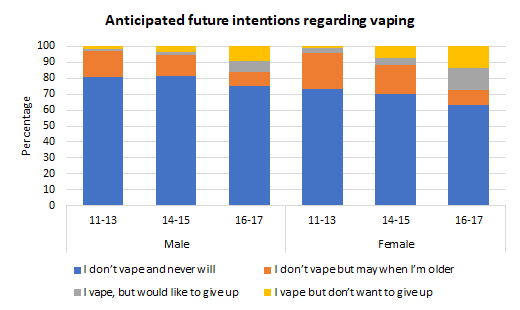
- Whilst the majority stated that ‘I don’t vape and never will’ (range 63% to 81% dependant on age and gender), sizeable percentages stated that ‘I don’t vape but may when they were older’ (range 13% to 23% for males and females aged 11-13 and 14-15 years, and less than 10% among those aged 16-17 years). Overall, 7% of males and 14% of females aged 16-17 years vaped but would like to give up, but 9% of males and 14% of females aged 16-17 years vaped and stated they did not want to give up vaping.
The Population Affected – Why Is It Important?
Tobacco is a unique product. It is the only consumable that, when used in the intended way, kills half of its users. This makes it one of the biggest causes of death and illness in the UK. Smoking causes around 80% of lung cancers, but can also cause cancer in many other parts of the body. Smoking also increases the risk of developing heart and circulation problems such as coronary heart disease, stroke, peripheral vascular disease and cerebrovascular disease. It also damages the lungs increasing the risk of bronchitis, emphysema and pneumonia, and other chronic obstructive pulmonary disease. Smoking can also cause or exacerbate numerous other health problems, and there are further risks caused by smoking in pregnancy and breathing in second hand smoke. Every year, there are around 64,000 deaths attributable to smoking in England. Smokers who die prematurely lose on average about 10 years of life.
There are also specific serious risks to the baby if their mother smokers during pregnancy (further specific details are given within Smoking in Pregnancy under Pregnancy and Maternal Health under Children and Young People). Second-hand smoke is very dangerous for anyone exposed to it, but it is particularly dangerous for children. Children exposed to second-hand smoke are at risk of ear infections, chest infections, bronchitis, pneumonia, breathing problems, allergies, asthma attacks and meningitis. Furthermore, nearly three quarters of children worry that their mum or dad will die because they smoke. Not only that, but if someone smokes in the household, children are three times more likely to smoke when they grow up. Most smokers start young (two-thirds before the age of 18 years).
The estimated to cost of smoking in England is in excess of £17 billion per year which is made up of £13.2 billion in lost productivity, £2.4 billion in healthcare, £1.2 billion in additional or earlier adult social care, and £283 million for costs associated with fires. In addition, it is estimated that people in England spend around £12 billion every year on legal and illegal tobacco products (just under £2,000 per smoker).
As smoking and deprivation are associated this acerbates the inequalities associated with poverty and deprivation. Smoking is the main contributor to health inequalities. Marmot in his original report in 2010 stated that smoking accounts for approximately half of the difference in life expectancy between the lowest and highest groups. Furthermore, as stated in Marmot’s ’10 years on’ report, it is more difficult for individuals to change unhealthy behaviours such as smoking when they are under stress caused by factors such as debt or poor housing.
An analysis commissioned by Action on Smoking and Health published in July 2021 using data for 2016/17 to 2018/19 with prices uprated to January 2020 prices, estimated across the UK that 17.9% of all households (4.98 million households in total) were living in poverty before tobacco expenditure was taken into account, but that this increased to 19.8% of all households (5.50 million households in total) once tobacco expenditure was included. In the subset of households where at least one person smoked, 21.2% of households (995,000 households in total) were living in poverty before tobacco costs were taken into account, but this increased to 32.4% households (1,521,000 households in total) once tobacco expenditure was taken into account. Among households where at least one person smoked, 26.6% of children were living in poverty before tobacco expenditure was taken into account (698,000 children in total), but this increased to 39.2% of children once tobacco expenditure was taken into account (1,029,000 children in total).
The health impacts of quitting smoking can be found in Smoking and Vaping Among Adults under Lifestyle Factors under Adults.
Whilst there is not enough evidence on the long-term harmful effects of using e-cigarettes, they are less harmful than smoking tobacco / cigarettes and can be used as an effective way to cut down smoking. The majority of adults who use e-cigarettes use them to cut down or quit smoking tobacco / cigarettes, or use them to stop them restarting smoking. However, among young people, particularly in the last couple of years, there has been an increase in the prevalence of vaping, and whilst there is a strong association between smoking tobacco and vaping among young people, the majority of young people who have tried vaping have never smoked tobacco / cigarettes or they tried vaping first before they tried smoking tobacco / cigarettes. So the pattern of use for e-cigarettes is different for adults and young people.
The Hull Picture
Recent locally produced estimates of smoking and vaping prevalence among young people are available from the local Health and Wellbeing Survey conducted in Hull secondary schools in Hull in 2024. There are no recent national estimates of the smoking prevalence among young people in Hull with the last national estimates produced in 2014.
A Vaping Survey was conducted across Hull in November and December 2022 among young people aged 11-17 years and this gives more recent information on both vaping and smoking tobacco, although the survey is not necessarily representative of Hull’s overall population.
Further information on both of these local surveys are available under Local Surveys Involving Young People within Surveys Conducted in Hull under Tools and Resources.
Smoking Cigarettes and Tobacco
From the Health and Wellbeing Survey 2024
Overall prevalence
From the local Young People Health and Wellbeing Survey of 2024 conducted in Hull secondary schools, 4.7% of males and 3.1% of girls reported smoking regularly or sometimes, with the overall prevalence of 3.9%. Prevalence increased with age, with fewer than 2% of pupils in year 7 to 9 smoking, compared with 5.1% of boys and 6.2% of girls in year 10 to 15.6% of boys and 7.2% of girls in year 11.
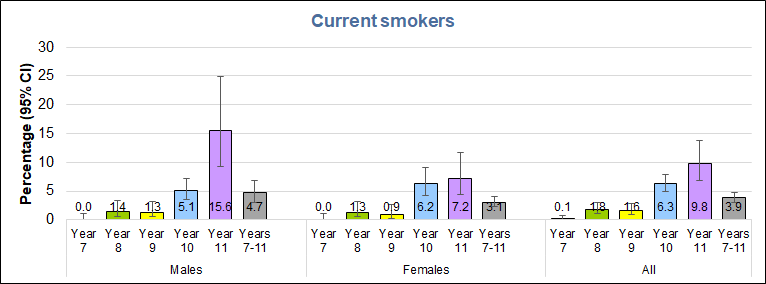
Based on the Office for National Statistics mid-year resident population estimates for 2023, there were 17,376 children of secondary school age in Hull. Applying the smoking prevalence by single year of age from the survey to the 2023 population estimates, it is estimated that there were around 673 young people in Hull aged 11-16 years who smoked.
Trends Over Time
Smoking prevalence among young people in Hull has decreased substantially over the last 16 years, from 12% of young people in 2008 to 3.9% in 2024, a decrease of 69%. The largest decreases were seen between the 2012 and 2016 surveys (31% decrease) and between the 2016 and 2024 surveys (49% decrease).
Comparison with England
It is possible to compare the prevalence in Hull in 2024 with that of England (for 2023) from NHS England’s Smoking Drinking and Drug Use Survey Among Young People. This national survey surveyed young people aged 11 to 15 years, so a similar age range to the Hull survey of secondary school students. Overall 3.3% of young people aged 11-15 years in England smoked, compared with 3.9% of year 7 to 11 pupils in Hull. Differences between Hull and England were greater among males. Among males 2.7% smoked in England, compared with 4.7% in Hull, while among females 2.8% smoked in England compared with 3.1% in Hull.
Influence of Deprivation on Smoking Behaviour
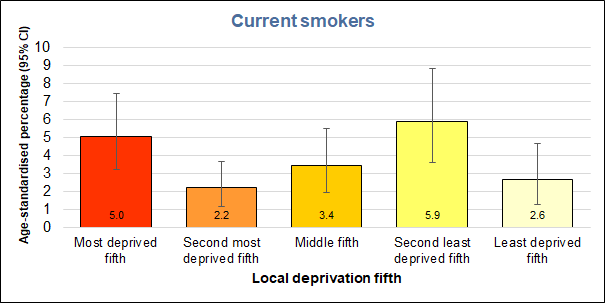
While the prevalence of smoking was twice as high among pupils living in the most deprived fifth of areas of Hull (5.0%) than among those living in the least deprived fifth of areas of the city (2.6%), there was no clear trend with deprivation, with the highest prevalence seen among young people living in the second least deprived fifth of areas (5.9%).
Smoking prevalence by selected subgroups
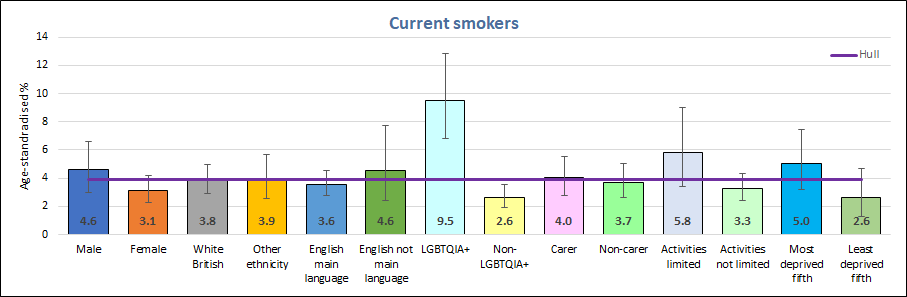
There were some large differences in smoking prevalence between various subgroups of pupils in the 2024 Health and Wellbeing Survey. The highest smoking prevalence rates were seen among pupils identifying as LGBTQ+, whose daily activities were limited by long-term illness or disability, as well as among pupils living in the most deprived fifth of areas of Hull. At 9.5%, smoking prevalence amongst pupils identifying as LGBTQ+ was 2.4 times higher than the average for Hull, the only subgroup with smoking prevalence was significantly higher than the Hull average. It was almost 3.6 times higher than among students who did not identify as LGBTQ+, the only subgroup with smoking prevalence significantly lower than the Hull average.
Easy to get cigarettes or tobacco
When asked how easy it was to get cigarettes or tobacco, 6.8% of males and 6.2% of females form the Young People’s Health and Wellbeing Survey 2024 said they found it easy. the percentages that found it easy to get cigarettes or tobacco rose rapidly with increasing school year. More young people reported that it was easy to get cigarettes or tobacco than reported smoking themselves.
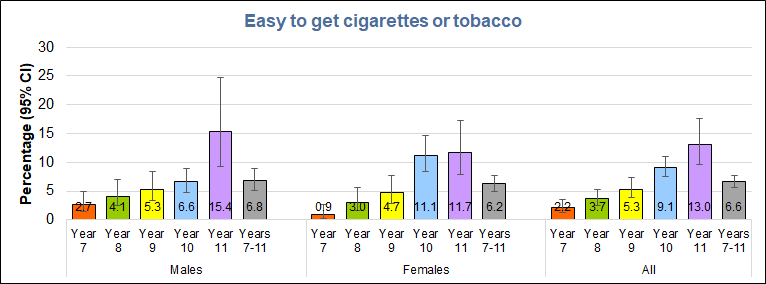
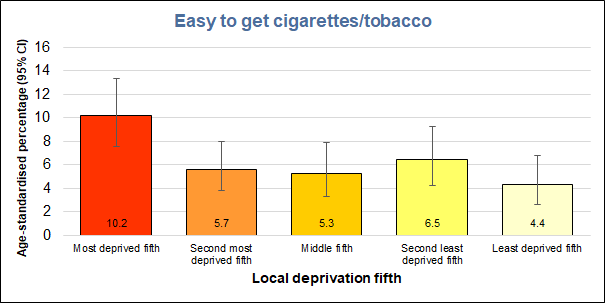
There were large differences in the percentages of pupils finding it easy to get cigarettes or tobacco according to the areas in which they lived. One in ten young people living in the most deprived fifth of areas of Hull reported finding it easy to get cigarettes or tobacco, more than double the percentage of pupils in the least deprived fifth of areas of the city.
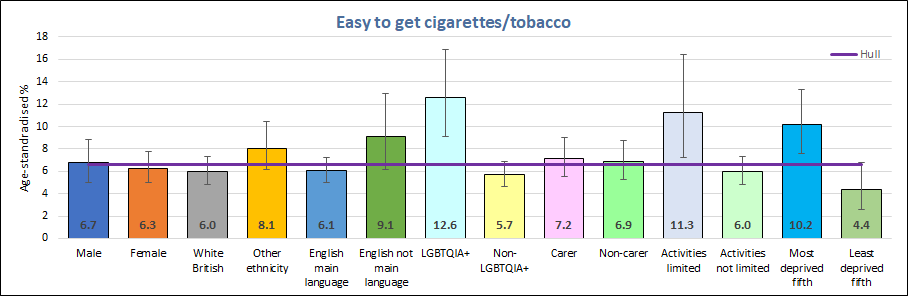
Three subgroups stood out with significantly higher percentages finding it easy to get cigarettes or tobacco than the average across Hull: young people identifying as LGBTQ+ (one in eight), young people whose daily activities are limited by long-term illness or disability (one in eleven) and those living in the most deprived fifth of areas of Hull (one in ten).
From the Health and Wellbeing Survey 2016
There were several questions about smoking that were asked about in the Young People’s Health and Wellbeing Survey 2016 that were not asked about in the 2024 survey, but that might still be of some interest, so they are presented in this section.
Quantity of Cigarettes Smoked
The majority of pupils who smoked had smoked 0-5 cigarettes per week. Two year 7 pupils smoked and provided the quantity smoked the previous week, and they had smoked 0-5 and 11-20 cigarettes in the last week. Five of the six year 8 smokers providing quantities had smoked 0-5 cigarettes the previous week and the sixth stated they had smoked 40+ cigarettes. Sixteen of the 32 year 9 smokers had smoked 0-5 cigarettes the previous week (five smoking 6-10, two smoking 11-20, six smoking 21-40 and three smoking 40+ cigarettes the previous week). Of the seventy year 10 smokers, 27 (39%) had smoked 0-5 cigarettes, 10 (14.3%) 6-10 cigarettes, 6 (8.6%) 11-20 cigarettes, 9 (12.9%) smoked 21-40 cigarettes, and 18 (25.7%) smoked 40+ cigarettes the previous week. Among the 46 year 11 pupils, 10 (21.7%) had smoked 0-5, 4 (8.7%) had smoked 5-10, 4 (8.7%) had smoked 11-20, 13 (28.3%) had smoked 21-40 and 15 (32.6%) had smoked 40+ cigarettes the previous week.
Exposure to Smoking and Smoke Within their Home
Over half of young people who lived in the most deprived and second most deprived fifth of areas of Hull lived with a smoker, and just under a third of these smokers smoked inside the home (equating to around 17% of these pupils overall exposed to smoke within the home). Among young people living in the least deprived fifth of areas of Hull, 28.5% lived with a smoker and just over one fifth of these smokers smoked inside the home (equating to 6.3% of these young people overall exposed to smoke within the home). Over all deprivation fifths, 45.0% of all young people lived with a smoker (32.3% did not smoke inside the home and 12.7% smoked inside the home).
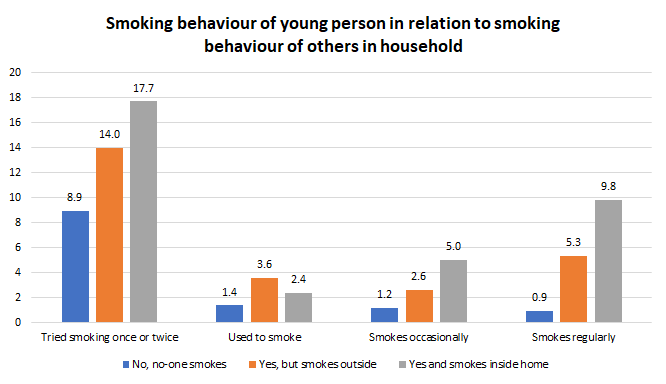
It is known that children growing up among smokers are three times as likely to become addicted to smoking themselves, and there was a strong association locally between whether the young person smoked and if other people within their household smoked.
Among young people who did not live with anyone in the household who smoked, 87.6% had never tried smoking not even a drag, 8.9% had tried smoking once or twice, 1.4% used to smoke but no longer smoke, 1.2% smoked occasionally and 0.9% smoked regularly. However, among young people who lived with one or more person who smoked, the rates of smoking were much higher. Among young people who lived with a smoker who smoked outside the home, 8.0% of young people smoked occasionally or regularly, but this was even higher at 14.8% if the household member smoked inside the home.
Source of Obtaining Tobacco and Cigarettes
Despite being illegal to sell cigarettes to anyone under the age of 18 years, 35% of boys and 24% of girls had bought cigarettes from shops. Just over one in five obtained their cigarettes from family members with around one in twelve being given cigarettes by their parents or carers. Three-quarters of girls and over half of boys obtained their cigarettes from friends.
Acceptability of Smoking
Pupils were asked if they thought it was OK for people of their age to smoke cigarettes or tobacco. There was a strong association with age, with around 1% stating it was OK to smoke among year 7 pupils increasing to 22% of male and 37% of female year 11 pupils.
Anticipated Future Intentions Regarding Smoking
Pupils were also asked about their anticipated future smoking behaviour. Among those who currently smoked 56% of males and 60% of females stated they would like to stop smoking, and among those who were non-smokers, 92% of males and 91% of females stated that they intended to never smoke.
Vaping Survey 2022
The Vaping Survey conducted during 2022 is not necessarily a representative sample of survey responders who live in Hull as only a few schools and colleges participated in Hull and it is possible that those that did participate at each school were not a representative sample of students due to the methodology employed for deriving the sample. Nevertheless, it is useful to examine the prevalence of smoking tobacco from this cohort.
Whilst the age groups are different from the Health and Wellbeing Survey 2016, the prevalence of regularly or occasionally smoking tobacco / cigarettes is much lower in the Vaping Survey 2022 at 0.5% and 0.7% among males and females aged 11-13 years respectively, and 7.7% and 11.12% among males and females aged 16-17 years respectively.
| Gender/age | Regularly | Occasionally | Used to but don’t now | Tried once or twice | Never not even a drag | Regularly or occasionally |
| Males 11-13 | 0.2 | 0.2 | 0.6 | 2.1 | 96.8 | 0.5 |
| Males 14-15 | 1.4 | 0.8 | 1.6 | 7.5 | 88.8 | 2.2 |
| Males 16-17 | 4.4 | 3.4 | 3.0 | 13.8 | 75.5 | 7.7 |
| Females 11-13 | 0.4 | 0.4 | 0.1 | 3.0 | 96.1 | 0.7 |
| Females 14-15 | 2.2 | 3.1 | 1.6 | 6.7 | 86.4 | 5.3 |
| Females 16-17 | 4.9 | 6.3 | 6.0 | 15.1 | 67.7 | 11.2 |
Among the 3,484 young people answering the question, across all age groups and both genders, 58 (1.7%) smoked regularly, 63 (1.8%) smoked occasionally, 58 (1.7%) used to smoke but do not now, 225 (6.5%) had tried smoking once or twice, and 3,080 (88.4%) had never tried smoking.
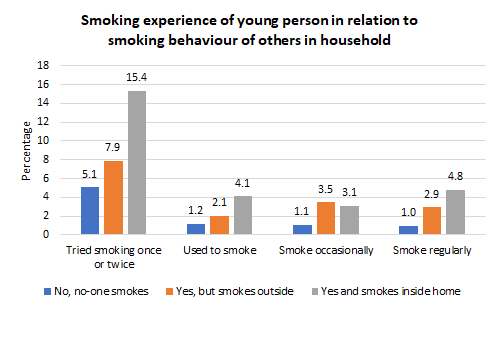
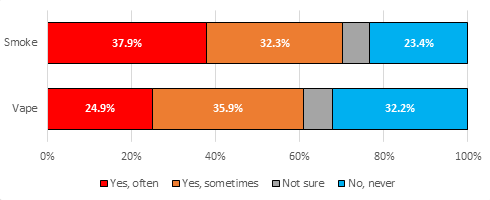
In Hull, 33.8% of the young people participating in the Vaping Survey lived with another person or others who smoked with 8.1% of them smoking inside the home and 25.6% of them not smoking inside the home. This was lower than in the Health and Wellbeing Survey 2016 where 45.0% of young people lived with a smoker (including 12.7% who smoked inside the home).
However, the smoking behaviour of the young people in the Vaping Survey was influenced by the smoking behaviour of others in the household. Young people were much more likely to have tried smoking, used to smoke, smoke occasionally or smoke regularly if there was a smoking in their household compared to if there was not a smoker in the household, and furthermore, if that household member smoked within the home then the young person was even more likely to have tried smoking or be smoke occasionally or regularly themselves. These percentages are lower than those noted from the Health and Wellbeing Survey conducted during 2016. This is likely to reflect slightly lower percentages of young people living with others who smoke as well as a change in behaviour among young people with regard to smoking tobacco / cigarettes.
Cost of Smoking in Hull
Action on Smoking and Health (ASH) have produced a Ready Reckoner (2022 edition) to calculate the cost of tobacco at local authority level.
In their 2022 edition of their Ready Reckoner, ASH estimate that there are 44,979 adult smokers aged 18+ years living in Hull (based on prevalence of 22.2% in 2018), and that the total cost of tobacco in Hull is £120.27 million each and every year. This includes the cost to the economy, healthcare, social care and to Fire & Rescue Services.
This does not include the estimated £87.5 million that smokers in Hull spend on tobacco products.
Further more detailed information can be found on the Smoking Among Adults under Lifestyle Factors under Adults, and at https://ash.org.uk/resources/view/ash-ready-reckoner
Attitudes to Smoking Tobacco
Further information is available under Surveys within Tools and Resources which gives the main report from the Young People Health and Wellbeing Survey 2016, information on smoking prevalence from the Adult Health and Wellbeing Surveys which include young people aged 16-24 years (the latest of which occurred during 2019), and qualitative research undertaken in 2008 and 2012 among secondary school pupils and young people aged 16-24 years which includes attitudes to smoking (Other Local Surveys and Qualitative Research).
Vaping
From the Health and Wellbeing Survey 2024
Vaping Prevalence
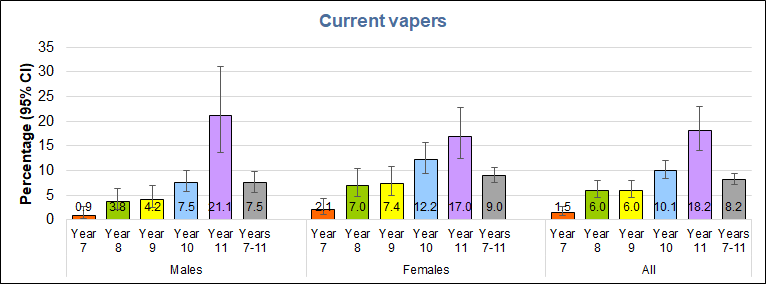
In the local Young People Health and Wellbeing Survey 2024, fewer than 2% of year 7 pupils overall vaped (although slightly higher among girls) but this increased with age to around 10% among those in years 10 and around 20% in year 11. The prevalence was generally higher among girls than boys, with the exception of year 11 pupils. The percentage of young people vaping in 2024 was higher for each sex and year group than the percentage smoking tobacco.
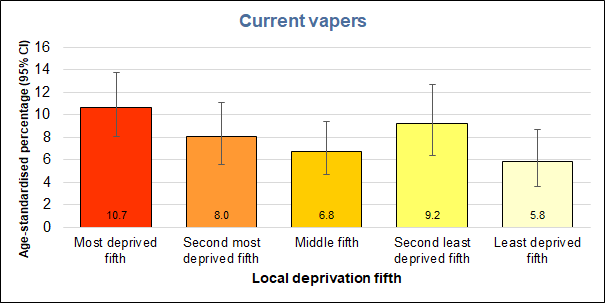
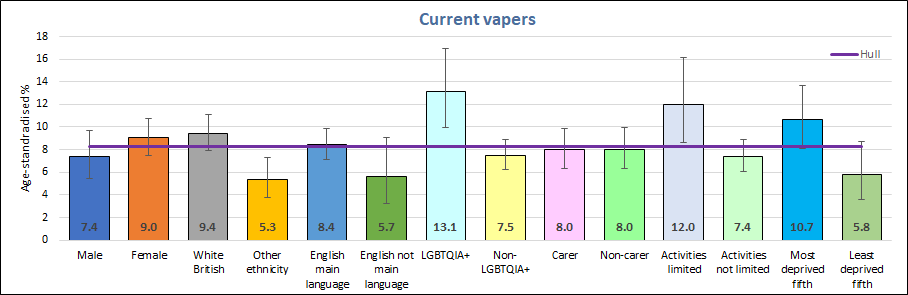
There were large differences by deprivation fifths in the percentage of young people vaping. More than one in ten young people living in the most deprived fifth of areas of Hull vaped (10.7%), 84% higher than the percentage of vapers amongst those living in the least deprived fifth of areas. The trend with deprivation was not totally consistent however, with those living ion the second least deprived fifth of areas having the second highest vaping percentage.
As with smoking, there was a large variation in vaping prevalence between various subgroups. The highest percentage of vapers were found among young people identifying as LGBTQ+, or whose daily activities are limited by long-term illness or disability, and those living in the most deprived fifth of areas (as mentioned above), with the percentages in the first two subgroups significantly higher than the Hull average. Every subgroup saw higher vaping prevalence than smoking prevalence, with the greatest differences seen for females and non-LGBTQ+ pupils (each three times more vapers than smokers) and White British pupils (2.5 times as many vapers than smokers). Carers, non-carers, young people with daily activities limited by long-term illness or disability, as well as those whose activities are not limited, those living in the most deprived fifth of areas and those living in the least deprived fifth of areas each had twice as many vapers as smokers.
Easy to get vapes
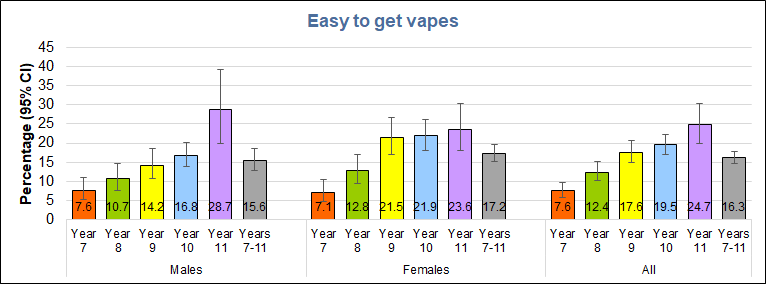
Despite being illegal to sell vapes to this age group, around one in six young people reported that they found it easy to get vapes, including one in thirteen in year 7, rising with school year to almost three in ten boys and almost one in four girls in year 11.
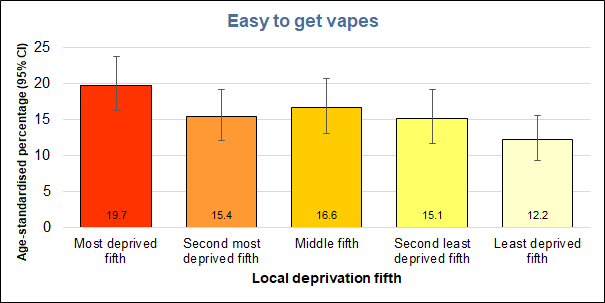
One in five students living in the most deprived fifth of areas of Hull found it easy to get vapes, 60% higher than for students living in the least deprived fifth of areas of the city, with a clearer trend by deprivation fifths than seen for vaping prevalence.
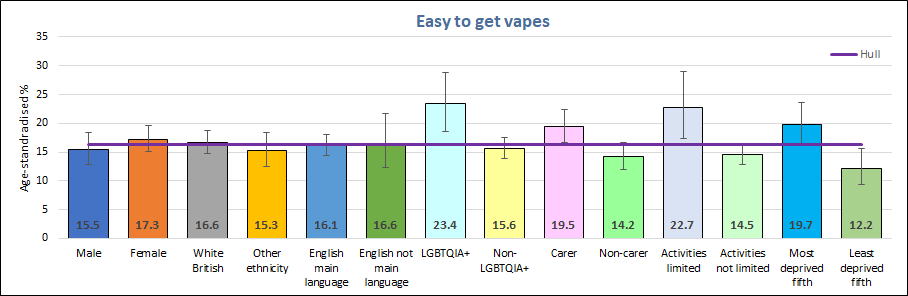
Apart from students living in the most deprived fifth of areas, three other subgroups stood out as finding it easy to get vapes, young people identifying as LGBTQ+ (23.4%), young people whose daily activities are limited by long-term illness or disability (22.7%), and young people with caring responsibilities (19.5%), with significantly higher percentages in each of these three groups finding it easy to get vapes than the Hull average.
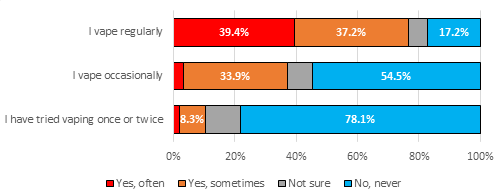
Association Between Smoking and Vaping
There was a strong association between smoking and vaping. It is possible to compare smoking prevalence with vaping among those young people who answered both questions. Among the 3,252 young people who had never smoked tobacco, 0.9% vape regularly and 1.3% vape sometimes, while 3.6% used to vape but no longer dis so (with a further 11.4% having tried a vape once or twice. Among the 120 young people who had tried smoking once or twice, 16.7% vaped regularly and 15% vaped sometimes while only 4.21% had never vaped (30.8% used to vape but no longer did so and 33.3% had tried a vape once or twice). Among the 31 young people who used to smoke tobacco but no longer do so, 38.7% vaped regularly and 9.7% vaped sometimes with 6.5% having never vaped (35.5% used to vape but no longer did so and 9.7% had tried a vape once or twice). Among the 30 young people who smoke tobacco sometimes, 53.3% vaped regularly and 26.7% vaped sometimes, while none reported never having vaped. Among the 52 young people who smoke tobacco regularly, 90.4% vaped regularly and 1.9% vaped sometimes with just 3.9% having never vaped. Overall, among those who currently smoke, whether regularly or sometimes, 87.8% also vape, while among non-smokers only 3.6% vape.
From 2016 Health and Wellbeing Survey
Acceptability of Using E-Cigarettes
Acceptance of e-cigarettes was higher than that for tobacco. Around 5% of year 7 pupils thought it was OK for young people their age to use e-cigarettes, but this increased to 11%, 21%, 34% and 45% among young people in school years 8, 9, 10 and 11 respectively. The percentages were similar among males and females for each school year except among year 11 pupils where more females thought it was OK to use e-cigarettes (51% versus 41%).
From Vaping Survey 2022
As mentioned earlier, the Vaping Survey conducted during 2022 is not necessarily a representative sample of survey responders who live in Hull as only a few schools and colleges participated in Hull and it is possible that those that did participate at each school were not a representative sample of students due to the methodology employed for deriving the sample. Nevertheless, it is an invaluable resource for looking at the current situation around vaping among Hull’s young people.
A summary of the results are given below, but further information is also available in the following report.
Knowledge of Vaping
Among all survey responders who attended a school or college in Hull, 10.5% of boys and 5.1% of girls aged 11 years stated they did not know what a vape or e-cigarette was, but this decreased to 1.0% among males and 2.1% among females aged 17 years. The individuals who did not know what a vape was or stated they were unsure, were not required to answer any further questions as they were all specific questions on e-cigarettes and vaping.
Exposure to Vaping
Overall, around two in ten (21.7%) young people stated ‘most’ people they knew vaped, four in ten (41.8%) stated ‘some’ people they knew vaped, one-quarter (26.7%) stated ‘hardly anyone’ they knew vaped, and only one in ten (9.7%) stated no-one they knew vaped. Older survey responders were more likely to know more people who vaped which is not surprising given that more of their peers vaped.
Overall, 59.4% of young people stated they had noticed a large increase in vaping among young people their age in the last year, and a further 28.7% stated they had noticed a small increase. Very few young people stated they had noticed ‘no’ increase.
Across all survey responders attending school or college in Hull, 37.0% lived with another person or other people who vaped, with the majority of these (22.7%) vaping inside the home (14.3% did not vape inside the home). Thus six in ten of those who had other people who vaped within the household were exposed directly to vaping inside the home.
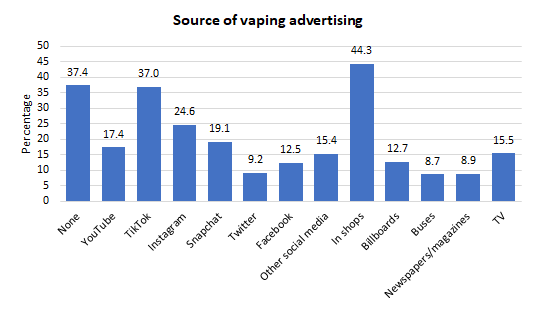
Opinions on Promotion of Vapes and Exposure to Advertising
Overall, two-thirds of 17 year olds thought that vapes were promoted towards young people, although the percentage was half that among 11 year olds. Depending on age and gender, 2-9% thought they were targeted towards children, 41-52% towards smokers, 9-15% towards non-smokers and 12-18% towards everyone.
The following chart illustrates the locations advertising vaping has been seen by young people across all age groups across Hull, although there were differences by age. Compared to 17 year olds, the 11 year olds were more likely to have seen no advertising (43.4% versus 35.9%) and to have seen advertising on YouTube (21.6% versus 15.1%), in the newspaper (11.1% versus 6.3%) and on television (21.8% versus 9.2%), whereas less likely to have seen advertising on TikTok (29.3% versus 40.5%), on Instagram (15.7% versus 25.7%), on Snapchat (16.4% versus 21.5%) and in shops (38.6% versus 49.3%) with no real difference by age for Twitter, Facebook, other social media, billboards, or on buses.
Opinions on Vaping
Young people were asked to tick all that applied to a number of statements relating to what they’d heard about vaping. The question was answered by all young people (except those who had stated they did not know what a vape was) so it includes a mixture of young people who have never vaped (the majority) and those who vaped regularly. The following chart illustrates the percentages who ticked the response to each question.
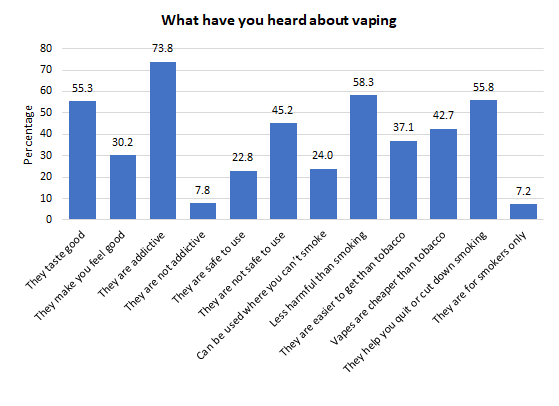
There were differences in what young people had heard depending on whether that individual had tried vaping or if they smoked tobacco / cigarettes occasionally or regularly.
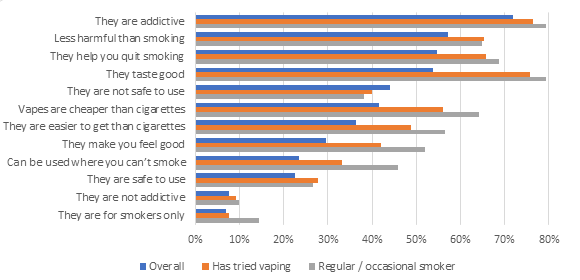
The majority of young people agreed that young people who vape like the taste and different flavours, and vape to look grown up. The majority also agreed with the statement ‘vaping is a waste of money’, and the majority agreed with statements comparing vaping with cigarettes/tobacco around vaping being preferable and less harmful. Around half agreed that vaping could help stop someone smoking cigarettes/tobacco, but the minority agreed with the statement ‘you should not vape unless you smoke cigarettes/tobacco’ (range 15-30% depending on gender and age group). There were differences in the responses depending on whether the young person had tried vaping or not and if they were a regular or occasional smoker or not.
Use of E-Cigarettes
The prevalence of vaping was much higher than the prevalence of smoking tobacco / cigarettes for both genders for all three age groups 11-13, 14-15 and 16-17 years in Hull’s Vaping Survey conducted during 2022.
The prevalence of vaping was also much higher among females compared to males, and increased markedly with age. Almost three in ten females aged 16-17 years regularly or occasionally used vapes compared to 17.3% for males. Twice as many females aged 14-15 years as males (10.1% versus 5.7%) vaped regularly or occasionally. Despite the high prevalence particularly among the older age groups, the majority of males and females for all three age groups had never tried vaping.
| Gender/age | Regularly | Occasionally | Used to but don’t now | Tried once or twice | Never, not even once | Regularly or occasionally |
| Males 11-13 | 1.0 | 1.6 | 1.7 | 10.4 | 85.3 | 2.6 |
| Males 14-15 | 2.9 | 2.7 | 2.9 | 13.3 | 78.1 | 5.7 |
| Males 16-17 | 11.4 | 5.9 | 3.8 | 18.3 | 60.6 | 17.3 |
| Females 11-13 | 1.7 | 1.6 | 1.1 | 9.5 | 86.0 | 3.3 |
| Females 14-15 | 6.1 | 4.0 | 4.6 | 12.7 | 72.6 | 10.1 |
| Females 16-17 | 18.6 | 9.8 | 4.3 | 16.0 | 51.4 | 28.3 |
Among the 3,290 young people answering the question, across all age groups and both genders, 179 (5.4%) vaped regularly, 117 (3.6%) vaped occasionally, 89 (2.7%) used to vape but do not now, 407 (12.4%) had tried vaping once or twice, and 2,498 (75.9%) had never tried vaping.
Influential Factors in Relation to Using Vapes
Young people who were exposed to vaping within the household were more likely to vape themselves. There was also a similar association between the vaping experience of the young person and whether or not others in the household smoked tobacco / cigarettes or not.
Three-quarters of all young people surveyed had never vaped and never smoked cigarettes / tobacco, 0.7% had never vaped but had tried smoking cigarettes / tobacco, 12.4% had never smoked cigarettes / tobacco but had tried vaping, and the remaining 11.8% had tried both vaping and smoking cigarettes / tobacco.
Despite many young people who had tried vaping had never smoked, there was a very strong association between vaping and smoking. Across all age groups and both genders, 99% of young people who had never vaped had never tried smoking cigarettes / tobacco. However, among young people who vaped regularly, only 19% had never tried smoking (23% smoked occasionally and 27% smoked regularly).
Among those who had never smoked, 86% had never vaped and a further 10% had only vaped once or twice. However, among young people who smoked regularly, 5% had never vaped, 8% vaped occasionally and 78% vaped regularly.
The majority of those who have tried vaping, did so before they tried smoking cigarettes/tobacco, particularly the younger age groups. Overall, excluding those who couldn’t remember, out of 630 young people, 449 (71.3%) had vaped first or had never smoked cigarettes/tobacco prior to vaping.
Vaping Experience
Whilst a high percentage of those who had tried e-cigarettes did not know whether it was disposable or re-chargeable, particularly among the younger survey responders who were more likely to have only tried vaping once or twice, of those who did know the type, the majority stated the type of e-cigarette was disposable.
Whilst girls tended to have a higher prevalence of vaping, boys had tried vaping for the first time at a younger age. Overall, 16% had tried vaping for the first time aged 9-11 years, 31% aged 9-12 years, 49% aged 9-13 years, 65% aged 9-14 years, 83% aged 9-15 years and 96% aged 9-16 years.
Among those who could remember, the majority of young people who had tried vaping had done so in the last year.
Of 353 pupils answering the question, across all age groups, 161 (45.6%) currently vaped everyday, 29 (8.2%) vaped 4-6 days a week, 43 (12.2%) vaped 1-3 days a week, 46 (13.0%) vaped 1-3 days a month, and 74 (21.0%) vaped less than monthly (excluding those who stated they no longer vape).
Survey responders were asked how much money they currently spend in a week on vaping. Of 593 pupils answering the question, 34 (5.7%) said they spent more than £15 per week, 53 (8.9%) stated £11-15, 69 (11.6%) stated £6-10, 66 (11.1%) stated £1-5 per week, and 371 (62.6%) stated nothing.
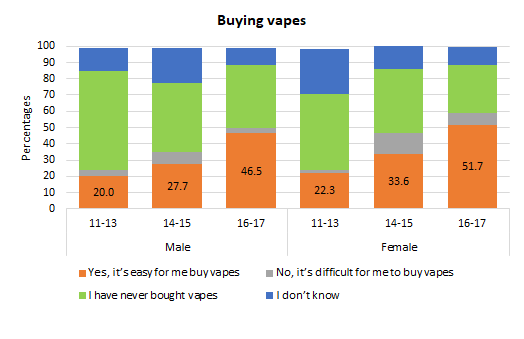
Buying Vapes
Across the local authority, significant percentages find it easy to buy vapes even among the youngest age groups despite it being illegal to sell vapes to under 18s.
The most popular brands used were Elux (56.3%); Elf Bars (29.9%); and Lost Mary (6.3%).
Overall, 71 (9.3%) of survey responders stated they had missed things like lunch or going out with friends so that they could afford to buy vapes.
Just over half of those answering the question relating to their parents or carers feelings on them vaping stated their parents or carers did not know they vaped, or they weren’t sure if they knew or didn’t know how their parents or carers felt about it. Of the remaining young people, 27.9% stated their parents or carers knew they vaped but that they did not mind, and 21.8% stated their parents or carers knew they vaped and that they were not happy about it.
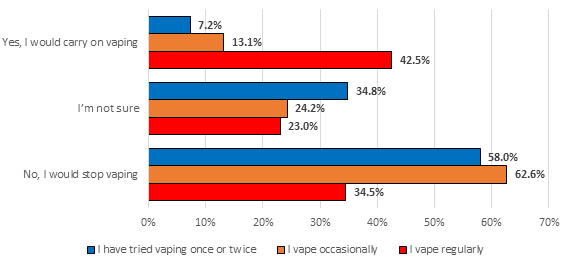
Of the 342 answering the question who did not state ‘I no longer vape’, 167 (48.8%) stated they would no longer vape if the vapes were only available in tobacco flavour, 88 (25.7%) stated they would carry on vaping, and the remaining 87 (25.4%) stated they were not sure if they would carry on vaping or not.
Unsurprisingly, the young people who vaped more frequently were more likely to carry on vaping if they were only available in tobacco flavour with 43% of those stating they would continue vaping among those who vaped regularly compared to 7% among those who had only tried vaping once or twice.
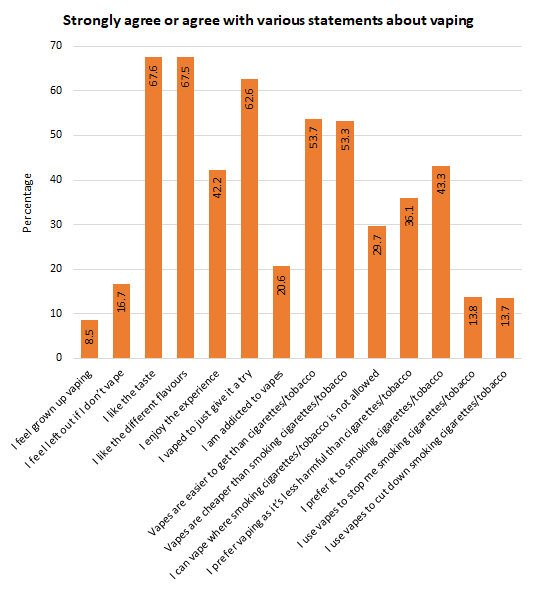
Survey responders who had tried vaping were given various statements around vaping and asked if they agreed or disagreed with those statements. The chart below illustrates the percentages who strongly agree or agreed with the various statements.
The highest levels of agreement were for ‘I like the taste’ and ‘I like the different flavours’ (both 67.5%), ‘I vaped to just give it a try’ (62.6%), ‘Vapes are easier to get than cigarettes/tobacco’ (53.7%) and ‘Vapes are cheaper than smoking cigarettes/tobacco’ (53.3%).
Overall, two in ten (20.6%) of those who answered the question stated that they were addicted to vapes. The lowest levels of agreement occurred for ‘I feel grown up vaping’ (8.5%), the use of vapes to cut down or stop smoking cigarettes/tobacco (both just over 13.5%) and ‘I feel left out if I don’t vape’ (16.7%).
Across all survey responders in Hull, 83 (11.1%) state that they often craved a vape or felt irritable if they hadn’t vaped for a while, 151 (20.1%) stated they sometimes felt like this, 444 (59.1%) stated they never craved a vape or felt irritable if they hadn’t vaped for a while, and the remaining 73 (9.7%) stated that they weren’t sure.
Not surprisingly, the percentage of young people who craved a vape or felt irritable if they hadn’t vaped for a while was higher among those who vaped more regularly (39% of young people who vaped regularly often felt a craving or felt irritable and a further 37% sometimes felt a craving or felt irritable).
Due to the strong association between smoking tobacco / cigarettes and vaping, the percentages who often or sometimes craved a vape or felt irritable if they hadn’t vaped for a while was high among those who occasionally or regularly smoked (70%) or who occasionally or regularly vaped (61%).
Anticipated Future Intentions Regarding Vaping
All survey responders (who knew what vapes were), were directly to the final question which asked them what statement best described them in relation to vaping. The options were: ‘I don’t vape and never will’, ‘I don’t vape but might when I’m older’, ‘I vape, but would like to give up’, and ‘I vape but don’t want to give up’.
| Statement | Males 11-13 | Males 14-15 | Males 16-17 | Females 11-13 | Females 14-15 | Females 16-17 |
| I don’t vape and never will | 80.9 | 81.4 | 75.3 | 72.9 | 70.2 | 63.2 |
| I don’t vape but may when I’m older | 15.8 | 13.2 | 8.4 | 23.1 | 18.2 | 9.1 |
| I vape but would like to give up | 1.6 | 1.9 | 7.0 | 2.8 | 4.3 | 14.2 |
| I vape and don’t want to give up | 1.7 | 3.5 | 9.4 | 1.3 | 7.4 | 13.5 |
Whilst the majority stated they do not currently vape and didn’t plan to vape in the future, a sizeable percentage of males and females aged 11-15 years stated they don’t vape but may when they are older. Furthermore, of those aged 16-17 years, 7.0% of males and 14.2% of females stated they currently vape but would like to give up and a further 9.4% of males and 13.5% of females currently vape in that age group but do not want to give up.
Further Information
Further information is available in our Vaping Survey report for Hull.
Strategic Need and Service Provision
The aims of SmokeFree Hull are to actively promote a smoke-free City, support quit attempts through pharmacotherapies and behavioural support and harness the wider public health workforce to deliver very brief advice to people they have contact with (“make every contact count”). The service works with other health care providers to access existing networks ensuring access to information and support is widely available. The Service uses a variety of methods to meet the needs of smokers and their families.
Preventing children and young people smoking is an important element of reducing prevalence and improving their health. Children and young people are twice as likely to become smokers if they live with a smoker. Local services work with children and young people to prevent them from starting or help them to quit through a dedicated Children and Young People Service.
The current adult SmokeFree Hull Service has a priority focus on people living in the most deprived wards (where smoking prevalence is the highest), pregnant women, and people with chronic obstructive pulmonary disease, coronary heart disease and mental health illness.
Hull Alliance on Tobacco is a multi-agency Alliance working collaboratively to reduce smoking prevalence. Helping smokers quit is one strand of the Alliance’s Plan which recognises other aspects of tobacco control are needed. This broader approach is supported by the Tobacco Plan for England, World Health Organisation, National Institute of Health and Care Excellence (NICE) and the Regional Tobacco Control Group.
In practice this means that in addition to helping people quit, Hull has effective regulation and enforcement through Trading Standards to reduce the availability of illicit tobacco, underage sales and enforcement of smokefree laws, work in partnership with the NHS as they become smokefree and support all areas through multi-media communication.
The core areas for HALT partners include mental health (parity of esteem), illicit tobacco, e-cigarettes, marketing, and children and young people (denormalising smoking). We want not smoking to be seen as the norm in all local communities. The HALT plan has three key priorities: smoking in pregnancy, supporting a smoke free NHS and health inequalities.
Resources
Hull’s Health and Wellbeing Surveys
NHS Digital. Health Survey for England 2018: https://digital.nhs.uk/data-and-information/publications/statistical/health-survey-for-england/2018
NHS England. Smoking, Drinking and Drug Use among Young People in England, 2023: https://digital.nhs.uk/data-and-information/publications/statistical/smoking-drinking-and-drug-use-among-young-people-in-england/2023
Action on Smoking and Health: https://ash.org.uk/home/
Action on Smoking and Health: Ready Reckoner. https://ash.org.uk/resources/view/ash-ready-reckoner
Estimates of Poverty in the UK Adjusted for Expenditure on Tobacco. Howard Reed, Landman Economics, July 2021. Report commissioned by Action on Smoking and Health. https://ash.org.uk/wp-content/uploads/2021/07/Smoking-and-poverty-July-2021.pdf
SmokeFree Hull: https://www.changegrowlive.org/smoke-free-hull/home
Bump the Habit: www.bumpthehabit.org.uk
Diary of a Chimney Kid. https://chimneykid.co.uk/
National Institute of Health and Care Excellence (NICE) Guidance NG29. https://www.nice.org.uk/guidance/ng209
Health Equity in England: The Marmot Review 10 Years on. https://www.health.org.uk/publications/reports/the-marmot-review-10-years-on
Action on Smoking and Health: Use of e-cigarettes among adults in Great Britain. https://ash.org.uk/resources/view/use-of-e-cigarettes-among-adults-in-great-britain-2021
Action on Smoking and Health: ASH resources on youth vaping. https://ash.org.uk/resources/view/ash-brief-for-local-authorities-on-youth-vaping
National Institute of Care and Health Excellence. Tobacco: preventing uptake, promoting quitting and treating dependence. NICE Guideline 209. https://www.nice.org.uk/guidance/ng209/chapter/recommendations-on-treating-tobacco-dependence#advice-on-nicotine-containing-e-cigarettes
Updates
This page was last updated / checked on 10 March 2026.
This page is due to be updated / checked in March 2027.